

-
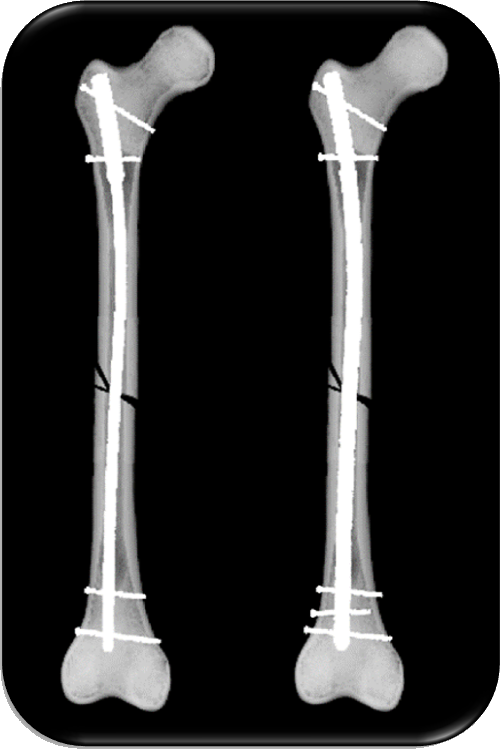
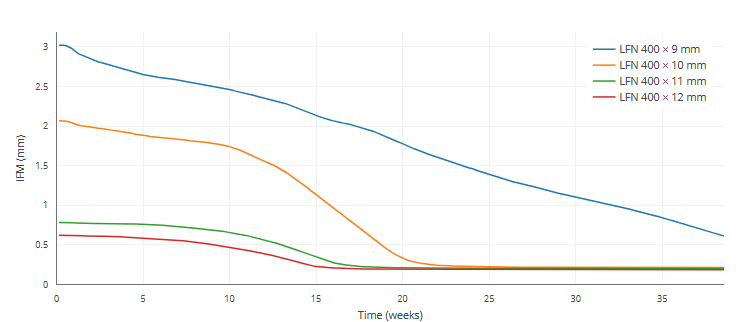
Minimizing shear and torsional movements at the gap promotes fracture healing.
-
Even a slightly bigger nail diameter results in disproportionately increased stiffness.
-
Greater system stiffness, in turn, results in less movement at the fracture gap.
-
The play of the nail inside the medullary cavity should be kept as small as possible.
-
Thus, choosing the largest possible nail diameter makes biomechanical sense, due to its superior stiffness.
References
-
Penzkofer et al. Influence of intramedullary nail diameter and locking mode on the stability of tibial shaft fracture fixation. Arch Orthop Trauma Surg 129, 525-531 (2009).
-
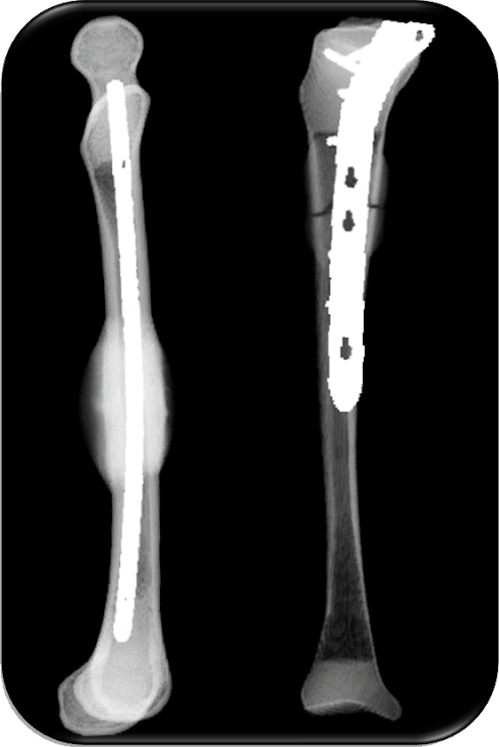
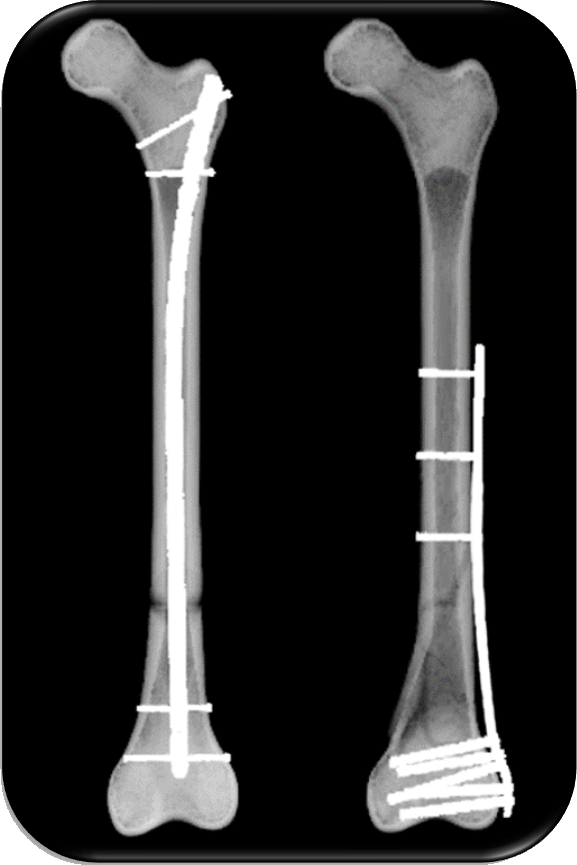
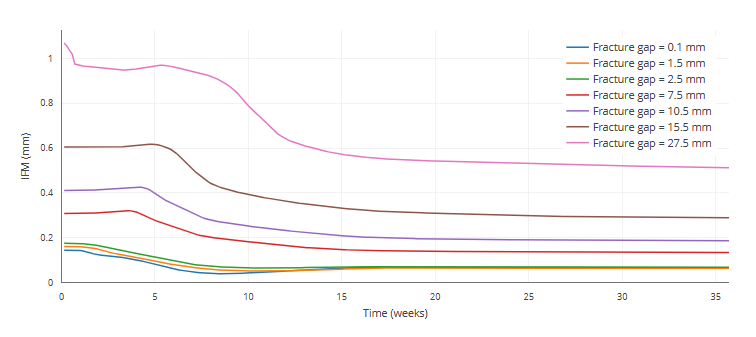
The quality of the fracture healing outcome and the rate of healing decreases with increasing fracture gap size.
-
Large fracture gaps can create critical size defects that supress healing and lead to non-unons.
-
A critical size defect might be defined as exceeding 1.5-3 times the diameter of the bone [2].
-
Larger osteotomy gaps lead to significantly more fibrocartilage and a lower amount of newly formed blood vessels in the gap healing area compared to osteotomy gaps of medium size.
-
From a clinical point of view, the use of operating techniques that avoid damage to the vascular system and allow reduction of the bone fragments, to achieve small fracture gaps, are important if we are to ensure proper fracture healing.
References
-
Claes et al. Influence of size and stability of the osteotomy gap on the success of fracture healing. J Orthop Res 15, 577-584 (1997).
-
Garcia et al. Rodent animal models of delayed bone healing and non-union formation: a comprehensive review. Eur Cell Matter 26, 1-12 (2013).