


-
Minimizing shear and torsional movements at the gap promotes fracture healing.
-
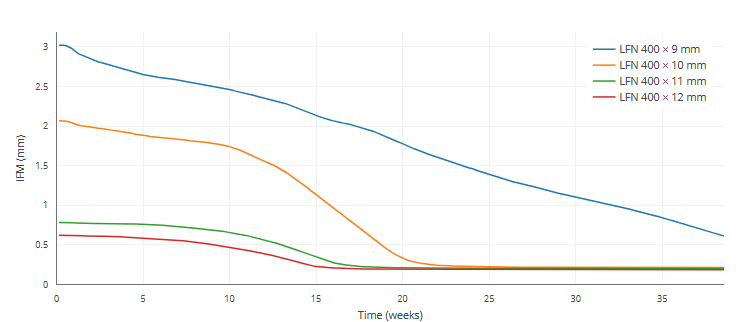
Even a slightly bigger nail diameter results in disproportionately increased stiffness.
-
Greater system stiffness, in turn, results in less movement at the fracture gap.
-
The play of the nail inside the medullary cavity should be kept as small as possible.
-
Thus, choosing the largest possible nail diameter makes biomechanical sense, due to its superior stiffness.
References
-
Penzkofer et al. Influence of intramedullary nail diameter and locking mode on the stability of tibial shaft fracture fixation. Arch Orthop Trauma Surg 129, 525-531 (2009).
-
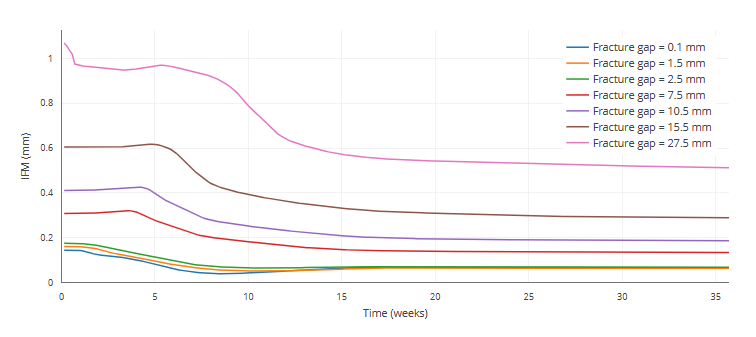
The quality of the fracture healing outcome and the rate of healing decreases with increasing fracture gap size.
-
Large fracture gaps can create critical size defects that supress healing and lead to non-unons.
-
A critical size defect might be defined as exceeding 1.5-3 times the diameter of the bone [2].
-
Larger osteotomy gaps lead to significantly more fibrocartilage and a lower amount of newly formed blood vessels in the gap healing area compared to osteotomy gaps of medium size.
-
From a clinical point of view, the use of operating techniques that avoid damage to the vascular system and allow reduction of the bone fragments, to achieve small fracture gaps, are important if we are to ensure proper fracture healing.
References
-
Claes et al. Influence of size and stability of the osteotomy gap on the success of fracture healing. J Orthop Res 15, 577-584 (1997).
-
Garcia et al. Rodent animal models of delayed bone healing and non-union formation: a comprehensive review. Eur Cell Matter 26, 1-12 (2013).
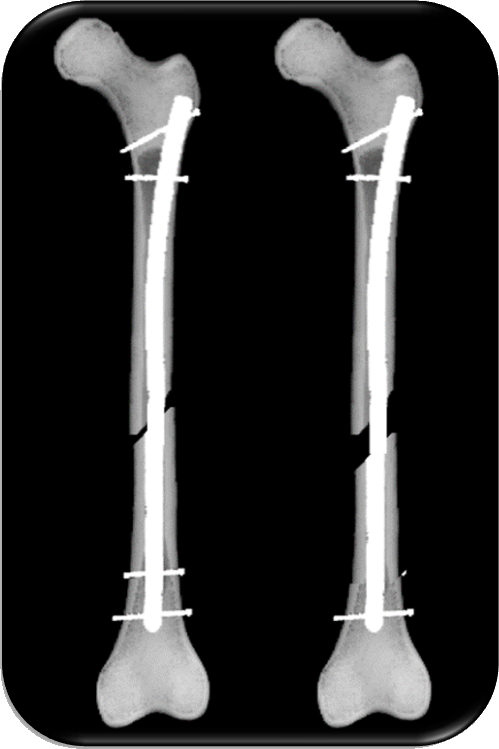
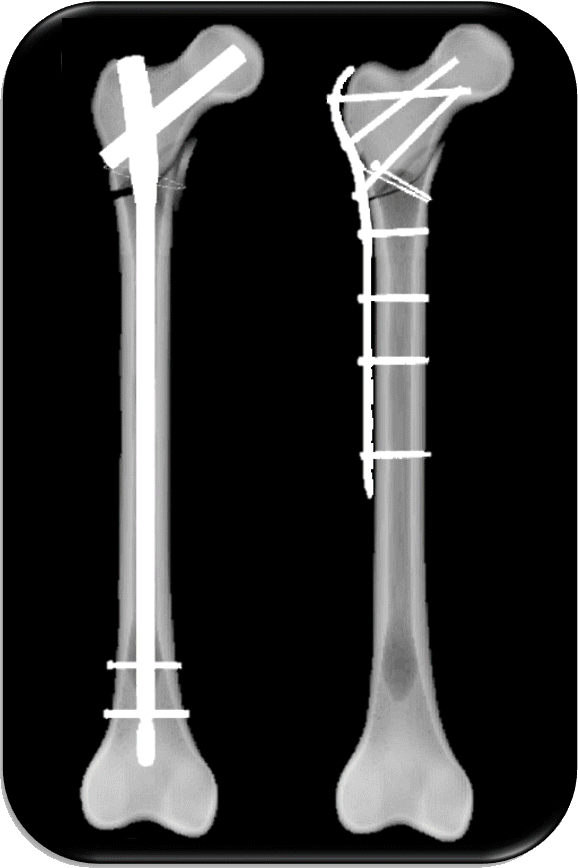
The intramedullary nail evolved from press-fit fixation to today’s nails that achieve stability through interlocking screws. Important landmarks in the development of nails are the introduction of flexible reaming, the transition from slotted to unslotted nail design, the introduction of “dynamization” of the nail and the use of titanium alloys as a new nail material [1].
- Choosing the largest possible nail diameter makes biomechanical sense due to the superior stiffness it provides [2].
- The play of the nail inside the medullary cavity should be kept as small as possible. Otherwise, the nail would be excessively loose in the cavity, and shear and torsional movements would be produced at the fracture gap.
- Minimizing shear and torsional movements at the gap will promote fracture healing.
- Greater system stiffness, in turn, results in less movement at the fracture gap.
- Suitable fracture patterns like axially stable fractures (e.g. A3) should be meticulously reduced and then compressed.
- Nail dynamization should be performed between three and six months after trauma [3].
References
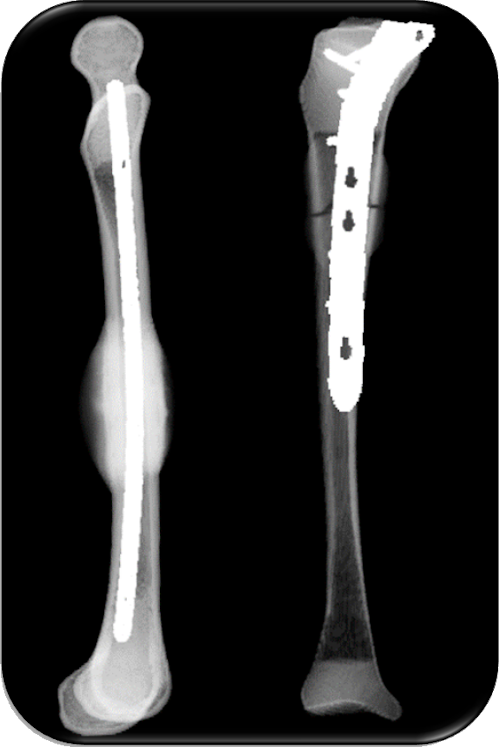
Umut Yavuz et al. Comparison of intramedullary nail and plate fixation in
distal tibia diaphyseal fractures close to the mortise. Ulus Travma Acil Cerrahi Derg, Vol. 20 (2014)Weihang Gao et al. Biomechanical comparison of intramedullary nail and plate osteosynthesis for extra-articular proximal tibial fractures with segmental bone defect. Front. Bioeng. Biotechnol., 11, (2023)
Cheng Ren et al. Comparison of intramedullary nailing fixation and percutaneous locked plating fixation for the treatment of proximal tibial fractures: A meta-analysis. Journal of Orthopaedic Surgery. 28(2) (2021)
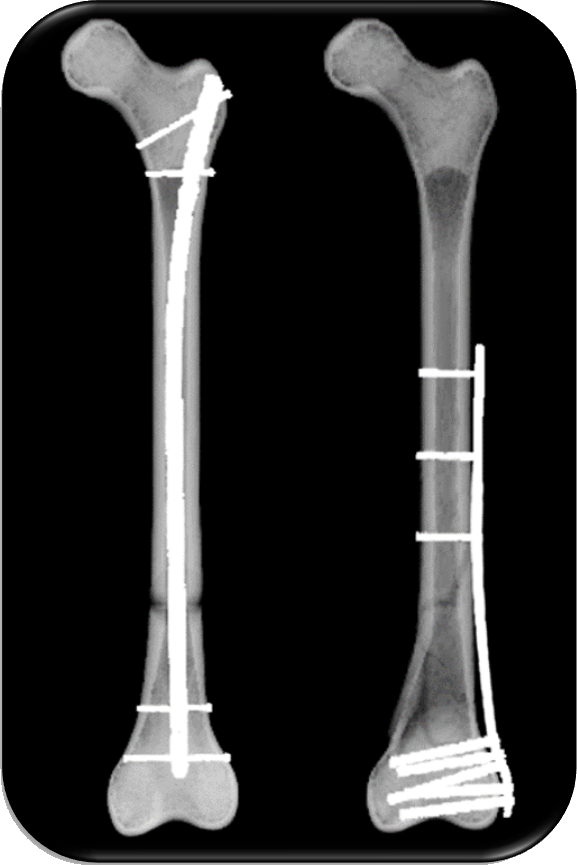
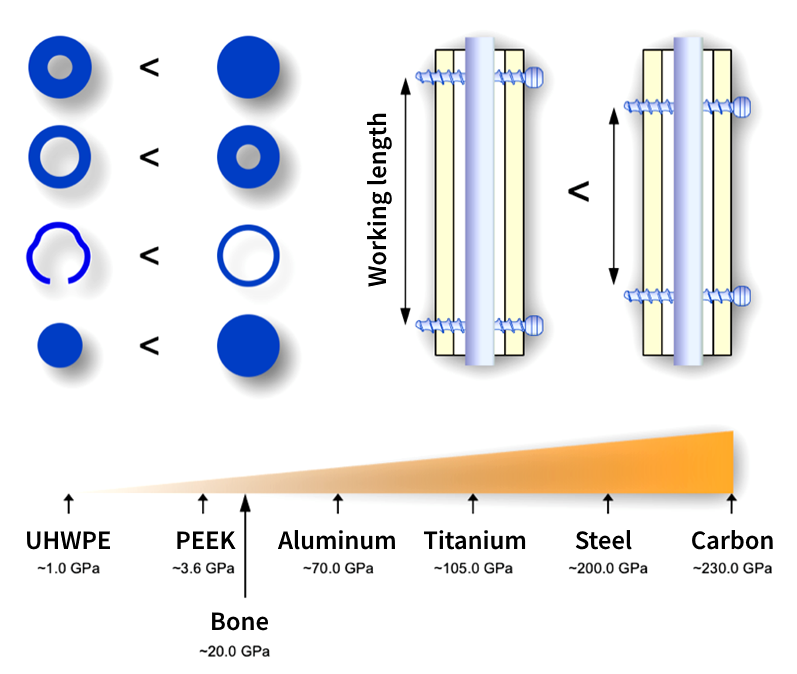
Working length:
- The plate working length should be as long as the fracture; if the working length exceeds the fracture length, the fracture will require longer to heal.
- A longer working length only reduces the plate load if the fracture gap closes and the load is shared between the implant and the bone. As healing progresses, the working length also affects the plate stress in the case of a comminuted fracture / fracture with a large gap.
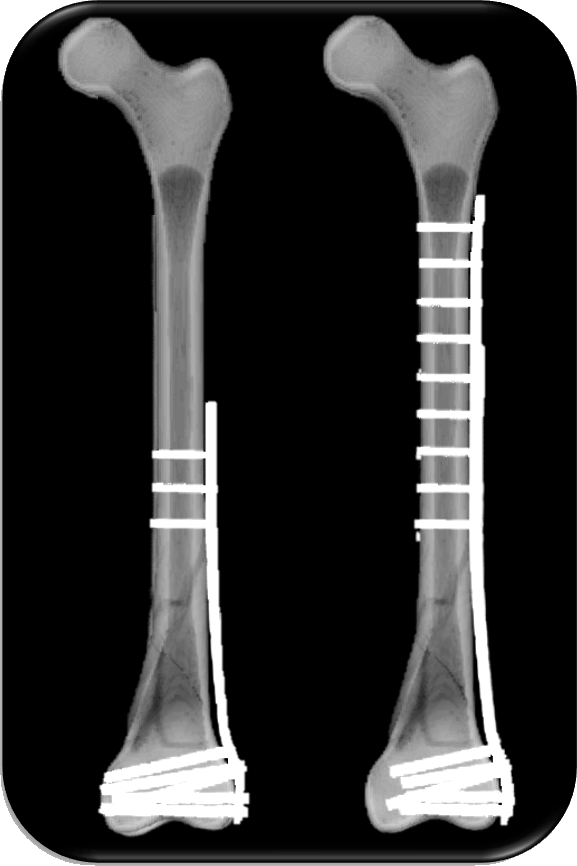
Plate length:
- According to Gautier et al., the length of a plate for a comminuted fracture should be at least 2-3 times the length of the defect [1].
- A longer plate does not harm fracture healing.
Min-Max-Principle:
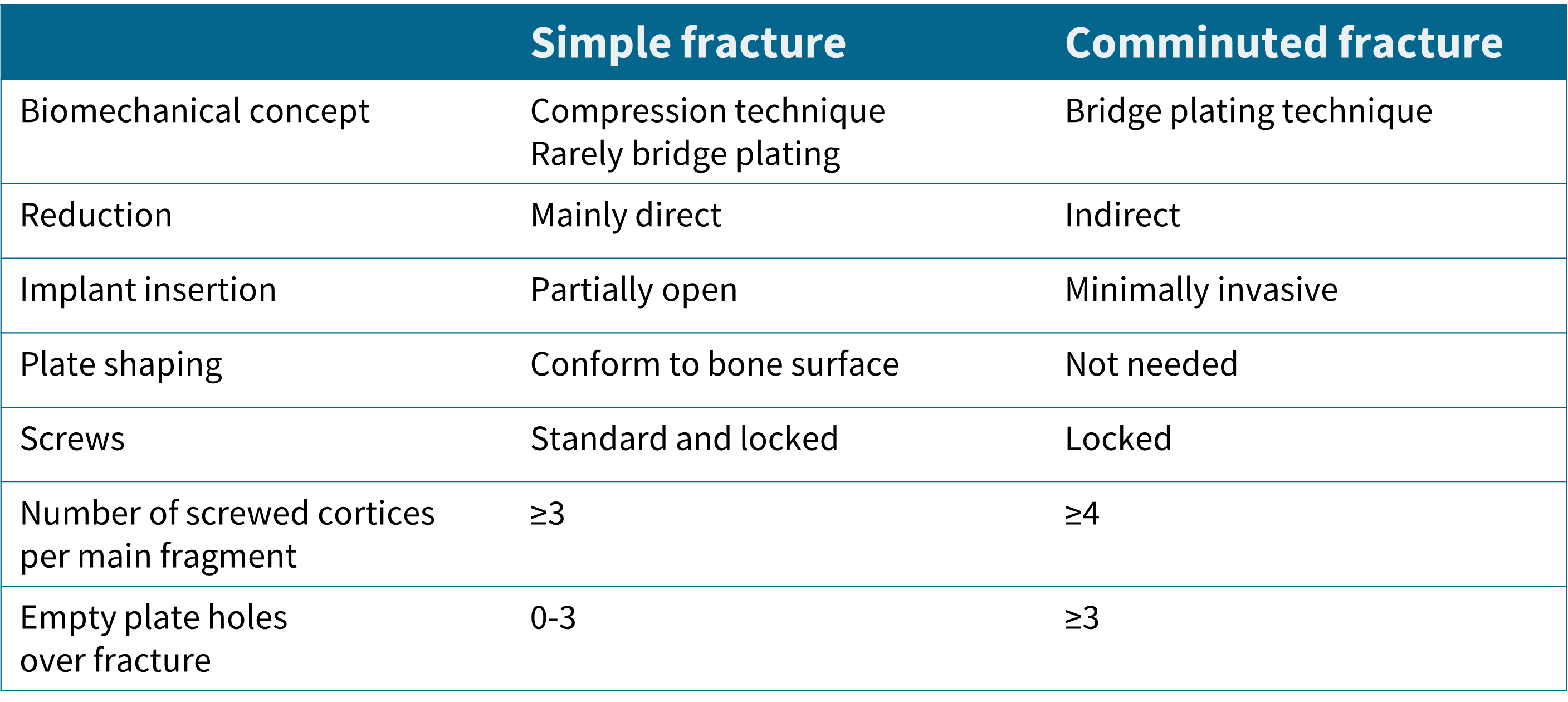
- Gautier and Sommer recommend holding screws in >3 for simple and >4 cortices for complex fractures [1].
Conclusive rules by Gautier et al.
References
- Emanuel Gautier, Christoph Sommer. Guidelines for the clinical application of the LCP. Injury 34, Supplement 2 (2003).